Elidel
Leitlinien
Deutsche S3-Leitlinie bestätigt topische Calcineurin-Inhibitoren als First-Line Therapie1**
Die deutsche S3-Leitlinie zur atopischen Dermatitis (AD) empfiehlt Calcineurin-Inhibitoren (TCI) wie Pimecrolimus als First-Line Therapie bei Unverträglichkeit und Nichtwirksamkeit von topischen Glukokortikosteroiden (TCS) und für empfindliche Hautbereiche.1**
Die S3-Leitlinie in Deutschland basiert auf den jährlich aktualisierten europäischen Leitlinien2, deren methodischen Arbeit dem S3 Status entspricht. Die deutsche AD-Leitlinie wurde somit von einem S2K- auf einen S3-Status angehoben. Die S3-Leitlinie deckt alle aktuell zugelassenen Systemtherapeutika ab und unterstützt bei der Bewertung individueller Diagnostik. Der hohe Stellenwert der topischen Therapie bestehend aus Basistherapie, antientzündlicher und antimikrobieller Therapie wird umfassend diskutiert und bewertet.
Die Autorengruppe hat aus Gründen der Übersichtlichkeit nicht alle Verfahren, die in der S3-Leitlinie diskutiert werden, in folgendem Stufenschema abgebildet:
Deutsche S3-Leitlinie:1 Stufenschema zur Therapie der atopischen Dermatitis (AD)

* Eine UV-Therapie kann ab Stufe 3, insbesondere im Erwachsenenalter, indiziert sein. Cave: keine Kombination von UV-Therapie mit Ciclosporin oder topischen Calcineurininhibitoren (TCI)
** First-line Therapie: In der Regel topische Glukokortikosteroide (TCS), bei Unverträglichkeit/Nichtwirksamkeit und an besonderen Lokalisationen (z. B. Gesicht, intertriginöse Hautareale, Anogenitalbereicht) topische Calcineurininhibitoren
*** Die zusätzliche Anwendung von antipruriginösen und antiseptischen Wirkstoffen kann erwogen werden.
Abbildung modifiziert nach S3-Leitlinie „Atopische Dermatitis“ (AWMF-Registernr. 013-027) (2023)
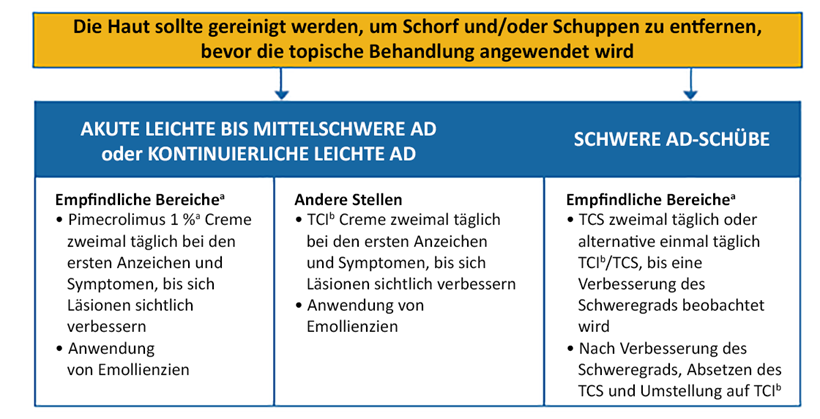
Als topische antientzündliche Therapien sind aktuell in Europa Glukokortikosteroide (TCS) und Calcineurininhibitoren (TCI) zugelassen. Im Folgenden aufgeführt die Empfehlungen der S3-Leitlinie für die antientzündliche Therapie1:
Empfehlungen für die antientzündliche Therapie

Abbildung modifiziert nach S3-Leitlinie „Atopische Dermatitis“ (AWMF-Registernr. 013-027) (2023)
Die Leitlinie finden Sie hier bei AWMF.org
Weltweit in Leitlinien empfohlen – Pimecrolimus bei AD von sensibler Haut
Aufgrund der breit aufgestellten Datenlage und dem günstigen Sicherheitsprofil wird Pimecrolimus in mehr als 50 Ländern eingesetzt3 und weltweit in Leitlinien zur Therapie der AD empfohlen. Im Folgenden finden Sie eine Auswahl internationaler Leitlinien zur AD-Behandlung. Wie in der deutschen S3-Leitlinie wird Pimecrolimus für die Behandlung von empfindlichen Hautbereichen und auch besonders bei Kindern empfohlen:
Asien-Pazifik4
- Das Expertenpanel zu atopischer Dermatitis der Asian Academy of Dermatology and Venereology (Asiatische Akademie der Dermatologie und Venereologie) entwickelte diesen Referenzleitfaden, um einen holistischen und evidenzbasierten Ansatz zur Behandlung von AD bei Asiaten bereitzustellen.
- Die Empfehlungen wurden auf Basis der Richtlinien des britischen National Institute for Health and Care Excellence und des schottischen Intercollegiate Guidelines Network bewertet.
Südafrika5
- Ein Gremium aus 12 Experten für AD erarbeitete einen praktischen Algorithmus für das Management im klinischen Alltag und Praxis für Kinder und Jugendliche
- Empfehlung von Pimecrolimus in der (Langzeit-)Anwendung, First-Line in sensiblen Arealen, auch < 2 Jahren
International6
- Ein internationales Panel von Dermatologie- und Allergieexperten aus China, Deutschland, Russland, der Türkei, Ukraine, Belarus, Jordanien und den Vereinigten Arabischen Emiraten verfasste ein Konsens-Dokument namens „Practical algorithm to inform clinical decision-making in the topical treatment of atopic dermatitis“ (Praktischer Algorithmus zur Entscheidungsfindung bei der topischen Behandlung von atopischer Dermatitis).
- Dieser Behandlungsalgorithmus kann bei der klinischen Entscheidungsfindung helfen und womöglich zu einer Entlastung der AD für den Patienten, ihrer Familien und der Gesundheitssysteme führen.
- Empfehlung bei leichter bis mittelschwerer AD:
- Pimecrolimus 1 % als bevorzugter topischer Calcineurininhibitor (TCI) zur Anwendung in empfindlichen Hautbereichen aufgrund des Wirksamkeits-, Verträglichkeits- und Selektivitätsprofils im Vergleich zu Tacrolimus.*
- Pimecrolimus und Tacrolimus werden für verschiedene Körperbereiche empfohlen.
- Topische Glukokortikosteroide (TCS) werden nur für die kurzzeitige Anwendung in Fällen schwerer Schübe empfohlen aufgrund ihrer Nebenwirkungen, wie die Verdünnung der Epidermisbarriere.
AD: Atopische Dermatitis; TCS: Topische Corticosteroide, TCI: Topische Calcineurin-Inhibitoren
Abbildung modifiziert nach: Luger T, et al. J Dermatol. 2021;00:1–10. DOI: 10.1111/1346-8138.15921
aDiese Bereiche umfassen den Kopf, das Gesicht (Augenlider und perioraler Bereich), Nacken, Axilla-Region, inguinale Falten und Genitalbereich. In diesen Bereichen wird eine Creme im Vergleich zu einer Salbe bevorzugt.
bPimecrolimus 1 % Creme bei Patienten ab 3 Monaten und älter, Tacrolimus 0,1 % Salbe bei Erwachsenen; Tacrolimus 0,03 % Salbe für Kinder. Pimecrolimus ist indiziert für leichte bis mittelschwere AD und Tacrolimus ist indiziert für mittelschwere bis schwere AD.
*Pimecrolimus ist indiziert für die Behandlung von leichter oder mittelschwerer atopischer Dermatitis für Erwachsene und Kinder, bei denen die Behandlung mit topischen Kortikosteroiden entweder nicht zu empfehlen oder nicht möglich ist. Pimecrolimus ist zweimal täglich auf die betroffenen Bereiche aufzutragen, bis die Anzeichen und Symptome der AD abgeklungen sind.
Pimecrolimus sollte so kurz wie möglich während eines Erkrankungsschubes angewendet werden. Die Behandlung sollte periodisch, kurzzeitig und nicht kontinuierlich sein.
Klinische Praxis: Wie kann eine steroidfreie Behandlung der atopischen Dermatitis optimiert werden? Tipps von Prof. Luger

* Elidel ist zugelassen für die Behandlung von Patienten ab einem Alter von 3 Monaten mit leichtem oder mittelschwerem atopischem Ekzem, wenn eine Behandlung mit topischen Kortikosteroiden entweder nicht angebracht oder nicht möglich ist, wie z. B. bei: Unverträglichkeit gegenüber topischen Kortikosteroiden; mangelnder Wirksamkeit von topischen Kortikosteroiden; Anwendung im Gesicht und Halsbereich, wo eine intermittierende Langzeitbehandlung mit topischen Kortikosteroiden nicht empfehlenswert ist.
Referenzen:
- S3-Leitlinie „Atopische Dermatitis“ (AWMF-Registernr. 013-027) (2023)
- Wollenberg, A et al. European guideline (EuroGuiDerm) on atopic eczema – part II: non-systemic treatments and treatment recommendations for special AE patient populations. J Eur Acad Dermatol Venereol. 2022 Nov;36(11):1904-1926.
- Mylan Pharmaceutical Pvt. Ltd. Data on File - IQVIA MIDAS Quarterly Audit Data. 2018.
- Chow S, Seow CS, Dizon MV, et al. A clinician's reference guide for the management of atopic dermatitis in Asians. Asia Pac Allergy. 2018;8(4):e41.
- Kannenberg SM et al., S Afr Fam Pract 2020; 62(1): e1–9.
- Luger T et al., J Dermatol 2021; 48(8): 1139–48; DOI: 10.1111/1346-8138.15921.
Weiterführende Inhalte
Servicematerial bestellen

Um kostenfrei Printmaterialien zu erhalten, teilen Sie beim Login bitte ihre Daten mit uns, damit wir die Materialien an Sie versenden können.
Dermatologische Erkrankungen
Die Haut – ein dynamisches Organ, das vom Säuglings- bis Seniorenalter von vielen Erkrankungen betroffen sein kann
Atopische Dermatitis

Unser Engagement: Viatris begleitet Patienten und Ärzte bei der Behandlung von Atopischer Dermatitis.